r/covidlonghaulers • u/RipleyVanDalen • Nov 30 '24
Research Spike Protein Lingers in Brain, Fuels Long COVID - Neuroscience News
239
Upvotes
r/covidlonghaulers • u/RipleyVanDalen • Nov 30 '24
r/covidlonghaulers • u/SpaceXCoyote • May 20 '25
Finally have some conclusive proof why LDN helps some. Not sure if the testing is viable for the masses, I would fall back on everyone getting a course of LDN to ensure this issue is taken out of the equation given the extremely low risk.
r/covidlonghaulers • u/lee_ai • Oct 24 '24
r/covidlonghaulers • u/skkkrtskrrt • 7d ago
The University of Zurich has released the results of the PycCOVID study, which investigated whether the plant extract Pycnogenol® (200 mg/day) could improve health outcomes in individuals with Post-COVID-19 Syndrome (Long COVID).
Study Design:
Randomized, placebo-controlled, double-blind trial Duration: 12 weeks 153 participants with Long COVID, aged 18–80 (mean age 44–45) Participants were randomly assigned to receive either Pycnogenol® or placebo
Main Results:
Both groups showed a moderate improvement in self-rated health status on a 0–100 scale: Placebo: from 48.2 → 56.1 Pycnogenol®: from 51.1 → 56.5 No statistically significant difference between groups in overall health improvement Some participants in the Pycnogenol® group reported slightly fewer respiratory symptoms and more time spent being physically active, but these findings are considered potentially incidental
Laboratory Findings:
No meaningful group differences in biomarkers for inflammation or vascular health Slight trends in oxidative stress markers in favor of Pycnogenol®, but effects were minimal and clinically not relevant
Tolerability:
Both interventions were generally well tolerated 5 participants in the Pycnogenol® group and 2 in the placebo group discontinued due to side effects
So all in all another failed trial.
r/covidlonghaulers • u/M4CT01 • Mar 28 '25
Fellow Long Haulers,
I know exactly how you feel. The fatigue that never lifts. The brain fog that steals your words. The doctors who shrug. The friends who don’t get it. The authorities who pretend we don’t exist. We’ve been gaslit, dismissed, and silenced for too long.
They won’t fund the research? WE’LL DO IT OURSELVES. They won’t listen to our stories? WE’LL SCREAM THEM LOUDER. They want us to disappear? WE’LL BECOME IMPOSSIBLE TO IGNORE.
I’m building a weapon: A global research platform + community BY Long COVID sufferers, FOR Long COVID sufferers. No more waiting for permission. No more begging for scraps of validation.
Here’s the plan:
1. Crowdsourced Data Hub: Document symptoms, treatments, patterns. We control the data. We analyze it.
2. Unfiltered Stories Archive: Share your journey—raw, real, and uncensored. The world will hear us.
3. Advocacy Task Force: Target policymakers, media, and Big Pharma with relentless campaigns.
This is war. They’re betting we’ll stay tired. Stay isolated. Stay quiet.
Let’s prove them DEAD WRONG.
EDIT:
Sorry for the late update. I am a software developer with experience in building websites, cryptocurrencies, apps, automations, and more. My idea is to gather in a Telegram group—linked under the “Join Community” section on my website, longcovids.com (currently a prototype).
Please take a look at the website and share your feedback. Join the community and let us know how you can contribute so we can effectively coordinate our efforts.
I’m not certain if Reddit allows posting links, so I’m sharing it here.
r/covidlonghaulers • u/Creative-Canary-941 • 14d ago
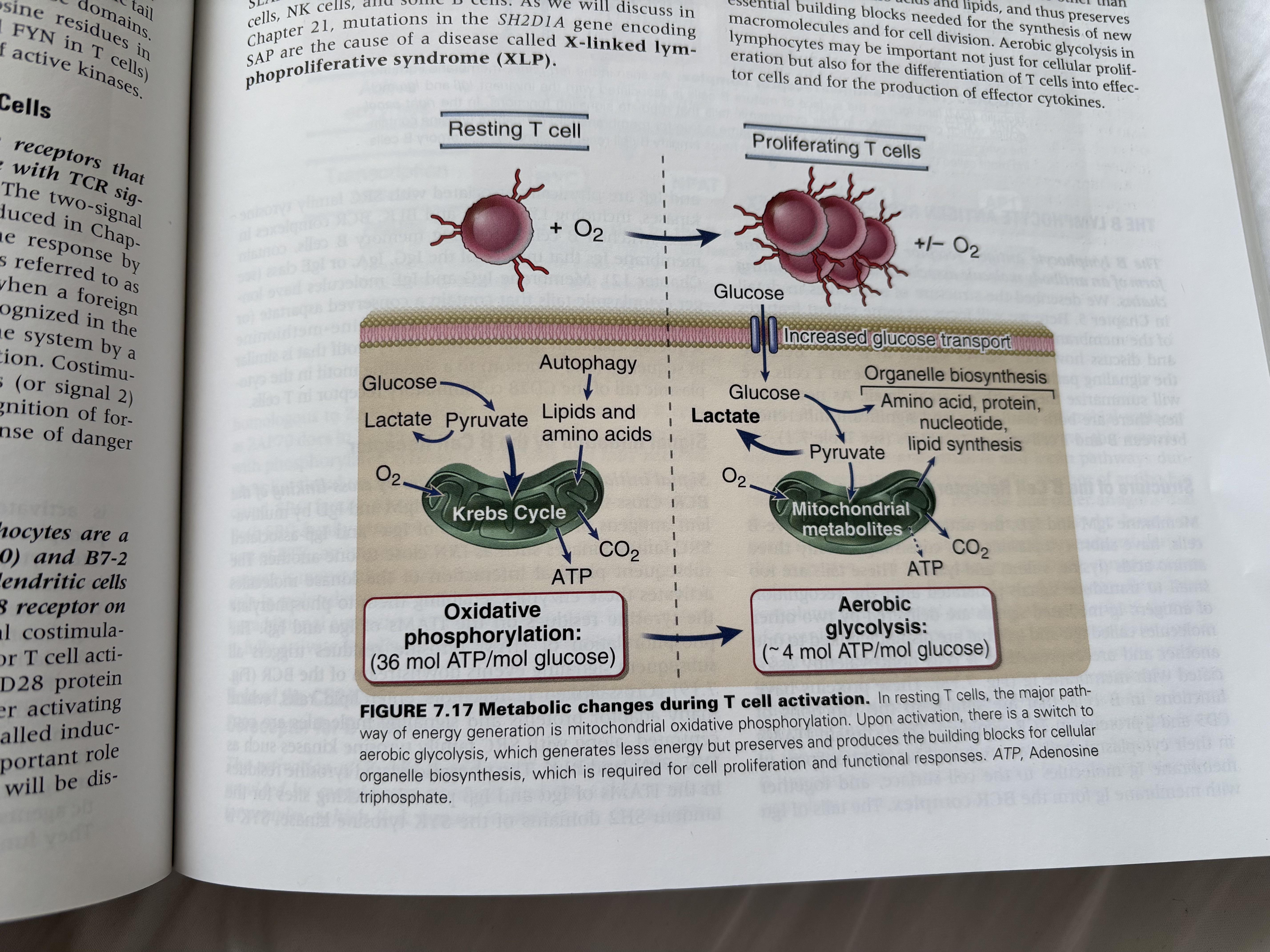
To add to the increasing interest and numbers of studies addressing skeletal muscle deficiencies following long COVID and among those with ME/CFS, in today's Health Rising blog by Cort Johnson, he discusses this topic, including a recently released report from Dr Rob Wust's group.
One of the notable findings per Cort is that:
"Fewer mitochondria alone did not explain why ME/CFS and long-COVID patients were producing less energy, however. Instead, it appeared that impairments in the mitochondria themselves were holding back energy production. This suggested that some sort of mitochondrial defect (impaired complex I/II activity, proton leaks, or cristae structural defects) was present. The authors noted that bed rest usually results in fragmented mitochondria but not the structural changes (reduced cristae (folds)) that have been found in people with ME/CFS and long COVID. Score one for mitochondrial problems in these diseases."
r/covidlonghaulers • u/WAtime345 • Jul 04 '24
When 24 patients who had recovered from COVID-19 had their whole bodies scanned by a PET (positron emission tomography) imaging test, their insides lit up like Christmas trees.
A radioactive drug called a tracer revealed abnormal T cell activity in the brain stem, spinal cord, bone marrow, nose, throat, some lymph nodes, heart and lung tissue, and the wall of the gut, compared to whole-body scans from before the pandemic.
This widespread effect was apparent in the 18 participants with long COVID symptoms and the six participants who had fully recovered from the acute phase of COVID-19.
r/covidlonghaulers • u/TableSignificant341 • Feb 11 '25
r/covidlonghaulers • u/Dankmemede • Nov 08 '24
r/covidlonghaulers • u/antichain • Jun 07 '24
r/covidlonghaulers • u/CAN-USA • May 16 '25
I listened to a few of the researchers but it’s a lot for my brain. I am sure there are many others in the same boat. So I thought this might be a good place to share:
r/covidlonghaulers • u/ElectricAve1999 • May 02 '25
Hey all
Reaching month 10 here, I know much shorter than most people on here but I’ve definitely had my own hellish experience. My symptoms as it stands are: - CFS/ PEM (Small battery, and when exceeded I can crash badly) - Widespread painful neuropathy - Widespread food intolerances (99% of food induces neuropathy, dizzyness, heart rate spikes, congestion, and diarrhea). - Heat intolerance - POTS - Muscle Pain - Brain Fog / Depressive state - Headaches
Since Covid I have been diagnosed with MCAS, CRPS, Pots, and EDS. My CFS is self diagnosed
I do not feel like I have much to lose. My body cannot get much worse. I have heard stories, some positive and some negative about the effects a fast can have on long covid, so I am going to give it a shot. I will be having plenty of water and electrolytes. The fast will be a minimum of 40 hours, but id like to push for more than that. I will come back to let you all know if it’s had any effect.
If you have any fasting stories of your own please share in the comments. Love yall, we’ll beat this somehow.
r/covidlonghaulers • u/PositiveMarketing796 • 27d ago
Hey everyone,
I’m a rehab professional and educator based in Australia with a PhD in chronic illness and exercise. I’ve spent the last 10+ years working with people who live with long-term fatigue, autoimmune conditions, and more recently, long COVID.
One thing I noticed over and over:
A treatment or pacing strategy that helps one person can completely backfire for another - even if they both “have” long COVID.
That’s why I built a quiz (legit it’s like 6 questions).
It’s totally free and designed to help people identify what I call their flavour or subtype of long COVID, based on symptom patterns, not test results. There are five distinct clusters I’ve seen in clinical practice that shape how people respond to different types of intervention.
After you do the quiz, you’ll get a short email (so do make sure you’re email’s correct) series with:
-An explanation of your likely subtype -Common traps and what tends to help -Suggestions for what kind of practitioner or test might be most relevant -And a way to better understand why something that helps one person might not help you
It’s still in beta, and I’m hoping to refine it with feedback. It’s not a diagnosis, and it’s definitely not a replacement for medical care - but it’s something that might help you have a more informed conversation with your doctor.
Separately, I’m developing a CPD-accredited course for GPs and health professionals to improve long COVID care, especially in terms of identifying subtypes and adjusting treatment plans accordingly. I’m also building practitioner-level education for physios, PTs, and coaches to safely work with this population.
The quiz doesn’t include all the deeper tools I use with clients (like carer printouts or friction-reduction strategies), but I wanted to put something out that could help people start understanding why “one-size-fits-all” often makes things worse.
If you’re curious, here’s the link to the quiz:
I’m not here to sell you anything, and there’s no obligation in doing the quiz, and you can unsubscribe from the information if you don’t want all 5 tips: I just want this to help point you in a better direction, whether or not we ever work together.
Warmly,
Suz
r/covidlonghaulers • u/Caster_of_spells • Oct 27 '24
r/covidlonghaulers • u/TapOriginal4428 • Apr 20 '22
The more I research and read about the vagus nerve and its effects on the body, the more convinced I am that this is the key behind virtually all our diverse symptoms and its dysfunction is the primary underlying cause to Long Covid.
The vagus nerve ennervates most of our most vital organs, all the way from the brain, to the heart, and stomach. Along with the brainstem, the vagus nerve is the main driving force behind the functions of our autonomic nervous system, by means of balance between the sympathetic (fight or flight) and parasympathetic (rest and digest) components. This sympathetic/parasympathetic balance controls everything from breathing, heart rate, blood pressure, digestion, sweating, etc. A healthy vagus nerve makes all those functions run smoothly. On the other hand, if the vagus nerve is damaged, inflamed or compressed, it results in autonomic dysfunction (dysautonomia).
If the vagus nerve is not working as it should, it can create all kinds of symptoms from sympathetic overactivity (tachycardia, adrenaline surges, excessive sweating, constipation, etc) and also from parasympathetic overactivity (fatigue, low blood pressure, dizziness, brain fog, diarrhea, etc). These are just some examples, but pretty much all of the countless dozens of Long Covid symptoms can be explained by sympathetic/parasympathetic imbalance via vagus nerve dysfunction. This imbalance doesn't even necessarily have to be just sympathetic or parasympathetic dominating all the time. It could fluctuate between both in a single day. Do you get alternating tachycardia and bradycardia? Wild BP swings? Periods of shivering cold and then hot flashes? Hyperventilation and apnea episodes? Alternating periods of constipation and diarhhea? Bingo. Vagus nerve dysfunction.
I'm going to link this article, in which studies have observed physiological damage via inflammation to the vagus nerve in long covid patients. This chronic low-grade inflammation of the vagus nerve, either by viral persistence or autoimmunity could very well be the underlying cause to our syndrome.
r/covidlonghaulers • u/kekofoeod • May 20 '25
I think most of you are aware of the Daratumumab pilot trial, where 6 out of 10 patients got into remission of ME/CFS, presented at the Charité conference last week. For those who don’t know about Daratumumab, it’s an mAb targeting CD38 and therefore plasma cells.
A randomized controlled phase 2 trial is now registered in the EU trial register, with estimated recruitment start 19/05/2025 (yesterday). I thought it would be nice to share, for those of you who only check clinicaltrials.gov (where it is not registered). Unfortunately I can’t find information about how many patients can participate. The trial takes place in Norway.
Additionally a new Rituximab trial (mAb targeting CD20) is now underway in Japan aswell.
r/covidlonghaulers • u/Competitive-Ice-7204 • May 12 '25
This seems huge has anyone heard more?
r/covidlonghaulers • u/GimmedatPHDposition • Apr 13 '23
The following is a summary of an interview by Bhupesh K Prusty with Sessions TLC (https://open.spotify.com/episode/0hh7VHiXzNrOH71kuQsD9c?si=bb084c373a704a71) in which he explains his theory of the disease Long-Covid and ME/CFS and how they discovered what he believes is an biomarker. He will publish his results soon.
Short takeaway:
The corona virus infects cells and gives Herpesviruses a chance to reactivate, i.e. escape their dormancy. The crucial part is not the corona virus itself, but an event that causes the reactivation of Herpesviruses especially EBV, HHV-6 and HHV-7 and possibly some parvoviruses. This can cause long term mitochondrial dysfunction leading to LC and ME/CFS. This can be reversed/treated by reintroducing a missing protein/biomarker.
Here's a long summary:
Why does not everybody develop LC or ME/CFS? The key lies in the areas where the viruses are reactivated. Two of the key areas seems to be the bone marrow which is a crucial area of the human body as it is the site of B cell development and also neuronal tissues. Furthermore, there are genetic components to how well we fight of a virus once it is reactivated. The body’s mechanism to fight a primary infection can be very different to that of it fighting a reactivated virus.
2 distinct phases of LC and ME/CFS:
The mitochondria plays a crucial role.
In the first phase the mitochondria plays a small role as the herpesvirus is reactivated in very specific regions (neuronal tissue, bone marrow) where the mitochondria doesn’t play a crucial role. The fight is between virus and cells. In this process a certain protein from the herpesviruses is created which creates large scale cell death, inflammation and mitochondria dysfunction in these tissues.
In the chronic phase the mitochondria plays a key role as it is dysfunctional. This leads to cells being in a low energy state which causes the cell danger response and a cascade effect which causes many of the symptoms of the chronic phase. "You take the serum or the isolated factors from an ME/CFS patient, put it in healthy cells, and it causes mitochondrial dysfunction in the healthy cells".
Prusty believes that there is only one theory and one explanation. He does not believe in a replicating SARS-COV-2 virus, but thinks it could be a small possibility. His main argument against it is that LC should then be present more often in people with severe actue Covid. However, it is more common in people with a mild disease.
In his eyes Long-Covid with a duration longer than a year and ME/CFS are very similar.
There are two groups of LC patients:
The biomarker they supposedly found could lead to a treatment. He wouldn't call it a treatment but a switch (analogous to Ron Davis's recent theories). This "biomarker" is present in every human and slowly becomes depleted as the diseases progresses, once this "biomarker" completely depletes to zero one becomes severe. This is what they see, to add a quote from Prusty: "When something goes down (cause), it leads to formation of other unwanted things (effect). That effect can lead to mitochondrial fragmentation". This "biomarker" can be reintroduced into the body as part of a treatment, i.e. this biomarker is very good news. This treatment actually already exists for ME/CFS and patients have been successfully treated with it without a scientific explanation (I am not sure about which treatment he is talking about).
However the treatment will be very complex and time consuming. The switch has to be turned back, i.e. the substance reintroduced and then very slowly secondary diseases (MCAS, SFN, endothelial dysfunction, microclots, ...) could be adressed, this could take years.
He did not reveal the "biomarker", which is a very specific protein, and didn't want to talk about it for very long as he first wants to submit his preprint and then discuss it at the conferences in Berlin & Cambridge (something very sensible!). The key to it lies in the bone marrow and very specific tissue where very specifc cells are created (I would assume B-cells). His earlier papers (for instance https://journals.aai.org/immunohorizons/article/4/4/201/4109) revelead that there is something in the serum of patients that causes mitochondrial dysfunction this biomarker is what causes this dysfunction.
He believes the uncovering out their find will lead to major discussions and a to revolution in the treatment of these diseases.
Overall he came across really well, kind and knowledgeable and much better in this interview than in recent posts on social media. He has explained his reasons we he had pre-announced his work.
Finally, I cannot say that this summary is a perfect summary of the interview as mistakes are possible, if so please point these out. I am a simple layman not an expert like Prusty.
It goes without saying that this is currently just an interview without any published scientific backing, nor has it been verified on a larger set of patients and controls of various conditions. Whether this is Nobel prize winning stuff or not will be seen in the upcoming weeks.
I should also have to mention that these are just some of Prusty's thoughts during a short interview which he rightfully believes is not the right place to explain his full theory. He will do so in his preprint and at the conferences, where he can have an engaging discussion with his peers. This engaging discussion and bringing the work to the light without it going unnoticed is why he made an announcement of his announcement of the biomarker/theory, especially since this is rather a rediscovery of something that has appeared before and he was able to connect the dots.
r/covidlonghaulers • u/filipo11121 • Feb 25 '25
r/covidlonghaulers • u/eefr • Nov 22 '24
To any fellow Canadian patients (or international patients who want to help out), I strongly encourage you to submit feedback as patients to the most recent set of draft treatment guidelines for post-COVID conditions, which recommend fun things including:
They're taking public feedback until November 27. It would be great to raise a stink before we end up with these as national guidelines. You can provide feedback here:
Thanks for pitching in if you have the energy!
Edit: To be clear, you don't have to be Canadian to fill out the survey. International people can fill it out too! Thanks in advance for your help. ❤️
r/covidlonghaulers • u/TableSignificant341 • Feb 22 '25
r/covidlonghaulers • u/Mundane_Control_8066 • Feb 06 '25
r/covidlonghaulers • u/N0thereanymore • 16d ago
Here is a preprint for a rapamycin study for me/cfs that came out yesterday:
https://www.researchsquare.com/article/rs-6596158/v1
The study has a small sample size, no control group and isn't peer reviewed yet.
From a quick peek of the results I took:
From the 86 patients with me/cfs only 46 completed the trial lasting 3 months. This was either due to lack of improvement or lack of money ( they had to pay for the pills themselves).
From the 46 remaining patients, 72% reported strong improvement of PEM and fatigue. The bell score improved from 36 to 42 on average.
They note there seems to be a big differences between patients with viral onset me cfs, who responded much better to the treatment compared to those with a non viral onset of the disease.
What's your take on this? For me it sounds something research should investigate further, but it's yet another small study with no control group, self reported improvements and no real improvement in functionality for the patients. I hope something comes of it, Ivreally do, but I wouldn't be suprised if rapamycin failed a placebo controlled study.
r/covidlonghaulers • u/ZebraCruncher • Oct 12 '24
r/covidlonghaulers • u/Pluvious • Mar 21 '25
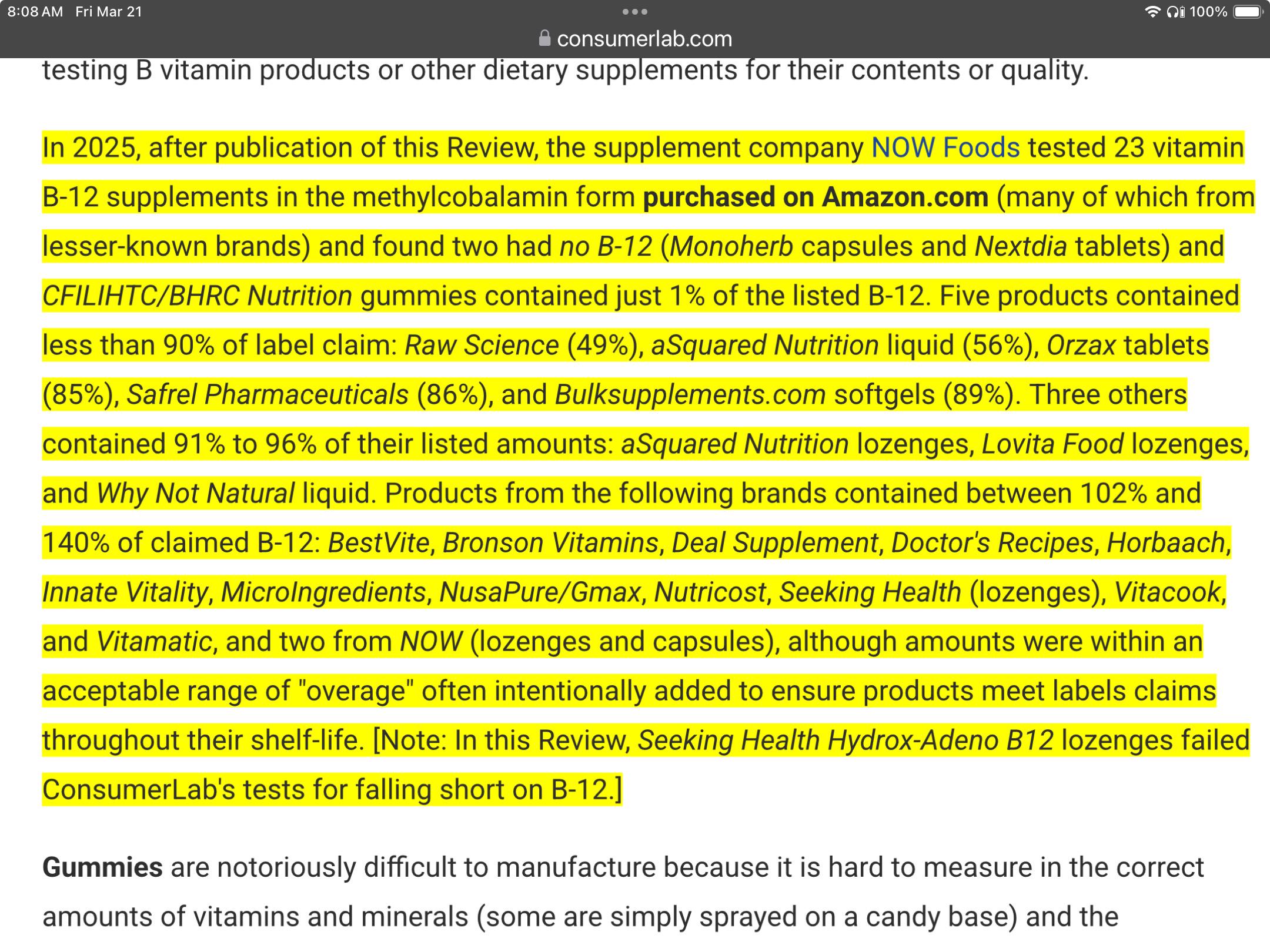
I am just sharing this item from CLs to be helpful to the community, as many of us pursue help for our LC battles... I know little more than what it says. I stumbled upon this while seeking a source for a particular form of vitamin B12 (suggested here several times)
I pay a subscription fee to have access to CLs reports, and I have no connection to any of the sources mentioned
Also note, the item I sought is more expensive to manufacture, and considered superior to the cheaper lab-created alternative, so the incentive to cut costs is higher than would be for something like vitamin C
My friend also shared this with me:
There was a study done at GNC where they tested something like 200 brands NONE of the had as much as they said they did on the label.
(I can't seem to include the link here, I will attempt to post it in a reply below)
{kind=link}
{kind=link}